Determining when to start routine mammograms can be pretty perplexing. Some health organizations suggest women begin screening at ages 40 or 45, while others recently recommended age 50. Plus, they don’t all agree on whether annual or biennial screenings are better.
This discrepancy partly stems from guidelines being tailored for women who are at average risk, meaning those with no cancer symptoms. However, breast cancer is prevalent, making it difficult to pin down who fits the “average” label and how to weigh the benefits and drawbacks of screening.
“Breast cancer isn’t just one type,” said Dr. Laura Esserman from the University of California, San Francisco. “So, how does it make sense to screen everyone the same way when their risks are so different?”
Esserman is spearheading research to better identify who falls into low or high-risk categories and to ultimately provide more personalized screening recommendations.
This year, over 320,000 women in the U.S. are expected to receive a breast cancer diagnosis, according to the American Cancer Society. Death rates have declined for many years, mainly due to improved treatments. Still, it’s the second leading cause of cancer-related deaths among women in the U.S., and diagnoses are gradually increasing.
For now, here’s what you need to know.
When to get a mammogram
The latest guidance from the American College of Physicians advises average-risk women aged 50 to 74 to have mammograms every other year. For those aged 40 to 49, they suggest discussing risks and benefits with a doctor, and if screening is pursued, to do so biennially.
This advice, released last month, caught many by surprise. Most other health organizations in the U.S. have encouraged women to start in their 40s. The U.S. Preventive Services Task Force recently adjusted its recommendation to begin biennial screenings at age 40 instead of 50.
The American Cancer Society has long recommended annual screenings for women aged 45 to 54 but allows for starting at 40. For women 55 and older, they can either switch to biennial screenings or continue annually.
Moreover, the new guidelines from the American College of Physicians suggest that doctors can check with women aged 75 and above about their wishes regarding routine screenings. In contrast, the cancer society believes there’s no reason to stop as long as they remain healthy.
Why don’t experts agree?
The rationale is that women at higher risk for breast cancer benefit more from frequent screenings. However, apart from well-known factors like the BRCA1 or BRCA2 genes, it’s challenging for women to gauge their actual risk. Age has traditionally served as a metric, given that the likelihood of breast cancer increases with age.
Mammograms are not foolproof. Sometimes they miss cancer, or aggressive tumors can emerge after a routine screening. Guidelines aim to balance early cancer detection against potential drawbacks, like the stress and discomfort that arise from further investigating spots that prove non-cancerous.
“We’re not saying there’s no advantage” to mammograms for women in their 40s, cautioned Dr. Carolyn Crandall from UCLA, who led the American College of Physicians report. But “there’s a narrower balance between the potential benefits and drawbacks for those aged 40 to 49.”
The American Cancer Society advises starting yearly screenings at 45 because research indicates that breast cancer rates for those aged 45 to 49 are closer to those for women aged 50 to 54 than for those in their early 40s, said Robert Smith, the society’s expert on early detection.
What’s lacking is a method to determine whether someone is prone to developing aggressive or slower-growing breast cancer, Smith observed.
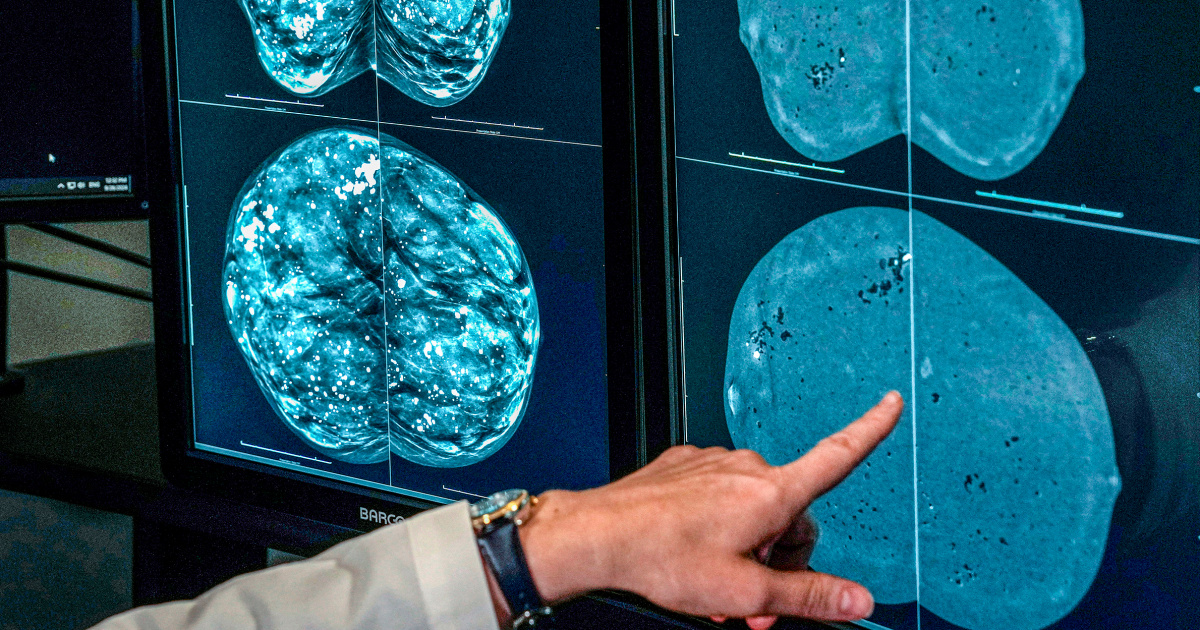
How dense breasts influence mammogram guidelines
Almost half of women over 40 have dense breast tissue, which can complicate tumor detection on mammograms and may slightly increase cancer risk.
Following a mammogram, women receive information about their breast density. Many experts are uncertain whether women with dense breasts would gain from additional ultrasounds or MRIs. However, the new American College of Physicians guidance recommends considering 3D mammography, known as digital breast tomosynthesis.
What’s next for breast cancer screening
Looking ahead, adding gene tests that go beyond the usual BRCA factors, alongside an assessment of broader risk indicators, may refine the most appropriate mammogram scheduling for women.
A recent study involving nearly 46,000 women—known as the WISDOM trial—classified women as low, average, elevated, or high risk based on age, genetic testing, lifestyle, health history, and breast density. This risk level then dictated whether they started mammograms at 50, went every other year, annually, or twice a year, with one screening via mammogram and another through MRI. Risk-based scans proved as effective as standard yearly screenings, as reported in JAMA. Surprisingly, about 30% of women categorized as high-risk through gene testing didn’t have familial history of breast cancer. While further research continues, Esserman hopes these initial findings will soon start shaping guidelines.
There are also AI tools in development aimed at evaluating a woman’s risk of breast cancer within the next few years by analyzing data from her mammograms, potentially helping to identify those who may need more or less frequent screenings.
Right now, women should discuss their family history of cancer, general health, and other risk factors with their doctors, like their childbearing history and age at first childbirth.
Regardless of the age at which they start or how often they choose to get screened, the key advice is to stay consistent, according to Smith from the cancer society: “Breast screening is most effective when done regularly.”