








Situation at a glance
The Bundibugyo virus disease (BVD) outbreak in the Democratic Republic of the Congo is quickly evolving, with ongoing transmission and more reported cases. By June 17, there were a total of 896 confirmed cases, along with 232 deaths, in the Democratic Republic of the Congo. Uganda reported 19 confirmed cases and two deaths by June 18, including one probable fatal case.
In Uganda, this outbreak is linked to the transmission that began in the Democratic Republic of the Congo, with indications of both imported infections and secondary transmission among contacts and healthcare workers. There have been no new cases reported in Uganda since June 5, 2026.
National authorities in both countries are working alongside WHO and other partners to roll out a comprehensive response strategy. A regional framework for preparedness is guiding activities throughout the African Region.
Description of the situation
Since the last disease outbreak news was shared on June 13, 2026, the confirmed cases and deaths in the Democratic Republic of the Congo have surged. A total of 915 confirmed cases have been reported, including 234 deaths, two of which are from Uganda. At least 88 patients have managed to recover from the disease; 78 from the Democratic Republic of the Congo and 10 from Uganda.
Update on the Democratic Republic of the Congo
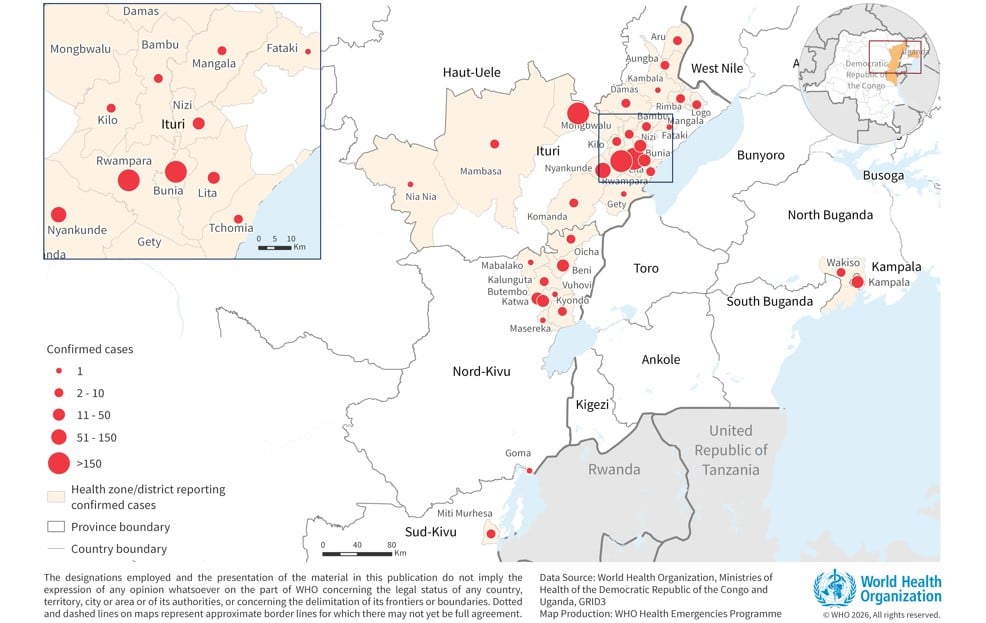
Since June 13, there have been 220 additional confirmed cases and 96 more deaths reported in the Democratic Republic of the Congo. This jump is partly due to enhanced testing capabilities that have cleared a backlog of samples. As of June 17, there were 896 confirmed cases with a case fatality rate of 26%, but this number is likely an underestimation since many deaths recorded prior to the official outbreak are still under review. Recoveries include 78 patients. Cases have been reported across 33 health zones in the provinces of Ituri, North Kivu, and South Kivu.
Most cases remain centered in Ituri Province, which alone accounts for 91.1% of confirmed cases, yielding a case fatality rate of 22.7%. The highest numbers of confirmed cases in Ituri are from health zones in Bunia, Rwampara, Mongbwalu, and Nyankunde. Although the epicenter is still Ituri, new cases have emerged from additional health zones, suggesting prior unnoticed transmission rather than a fresh wave of infections. Epidemiological reports suggest transmission may have been active in certain areas weeks prior to confirmation. Of the total cases, 17 are pending classification by health zone.
As of June 17, 6,367 contacts have been identified and are being monitored across the affected provinces. A total of 4,525 of these contacts have been followed, yielding follow-up rates around 70% in Ituri and North Kivu, while South Kivu has a 100% follow-up rate.
The outbreak is occurring in a complex humanitarian setting, marked by displacement and mobility among populations lacking basic services like food, clean water, healthcare, and shelter. These compounded challenges increase risks in overcrowded camps for internally displaced individuals. Security issues affecting healthcare facilities add operational hurdles, making it difficult for response teams to access affected areas, which could hinder surveillance and control efforts. Thus, local leadership and community-centered response efforts are crucial now.
Update on Uganda
The last confirmed case in Uganda was reported on June 5, 2026. As of June 18, there have been a total of 19 confirmed cases, which include two deaths linked to imported cases and one probable fatality. Of those confirmed cases, 14 were imported, while five resulted from secondary transmission in healthcare settings. These cases emerged from Kampala and Wakiso districts, which are part of the Kampala Metropolitan Area. So far, there’s been no evidence of community transmission in Uganda. Risks appear tied to healthcare settings and cross-border exchanges. After reviewing cases, the number of affected healthcare workers has been adjusted from five to four, with 10 total recoveries reported so far.
Of the 826 identified contacts as of June 18, 122 are actively being monitored, while 694 have completed their follow-up period.
Epidemiology
Bundibugyo virus disease, often fatal, is caused by the Bundibugyo virus, part of the Orthoebolavirus species. It’s zoonotic, with fruit bats believed to be the primary reservoir. Human infections typically happen through close contact with infected wildlife. The virus spreads among people through direct contact with bodily fluids or contaminated surfaces, particularly in healthcare settings lacking adequate infection control, and during unsafe burials.
The incubation period for this disease can be from two to 21 days, with individuals only being infectious after showing symptoms. Early signs—like fever and muscle pain—are non-specific, making clinical diagnoses tricky and potentially delaying identification. The disease can escalate quickly to more severe symptoms, including organ dysfunction. Case fatality rates from previous outbreaks in 2007 and 2012 in Uganda and the Democratic Republic of the Congo were notably high, at 30% and 50% respectively.
It’s difficult to distinguish BVD from other febrile illnesses, like malaria, without lab confirmation through PCR or other assays. Outbreak management hinges on rapid identification and isolation of cases, effective contact tracing, safe burial practices, and community engagement, especially since there are no approved vaccines or specific treatments available for BVD.
Public health response
Health authorities in the affected regions, along with the WHO and partners, are putting extensive public health measures into place. This involves executing a continental response plan, engaging donors, and mobilizing resources to fill critical funding gaps and sustain operations in at-risk areas.
WHO risk assessment
On June 6, 2026, the WHO reassessed the outbreak risk associated with Bundibugyo virus disease, focusing on new information. The risk remains high for countries that share borders with the Democratic Republic of the Congo and Uganda. The situation in the Democratic Republic of the Congo is assessed as very high due to ongoing transmission and the spread into new health zones, increasing the potential for wider dissemination.
In Uganda, the risk is still considerable due to confirmed cross-border cases and links within the eastern Democratic Republic of the Congo and western Uganda corridor, historically impacted by Ebola outbreaks. Overall, the risk assessment for land-bordering countries is high, while the broader African region and global levels are considered low.
WHO advice
The WHO currently does not recommend any travel or trade restrictions related to the Democratic Republic of the Congo or Uganda based on existing data. They are continuously monitoring and verifying measures related to this health emergency.
The Temporary Recommendations underline the necessity for coordinated outbreak control, enhanced border collaboration, and ongoing surveillance to manage the situation effectively. The WHO has formed several technical advisory groups to evaluate potential vaccines and treatments for BVD. Recommendations from these groups are available in related releases.
Further information
Current outbreak status:
Epidemiological updates and situation reports.
Clinical management, infection prevention, and training.
Past Bundibugyo virus disease events, Democratic Republic of the Congo (2012).
Background and reference information available from the WHO.







