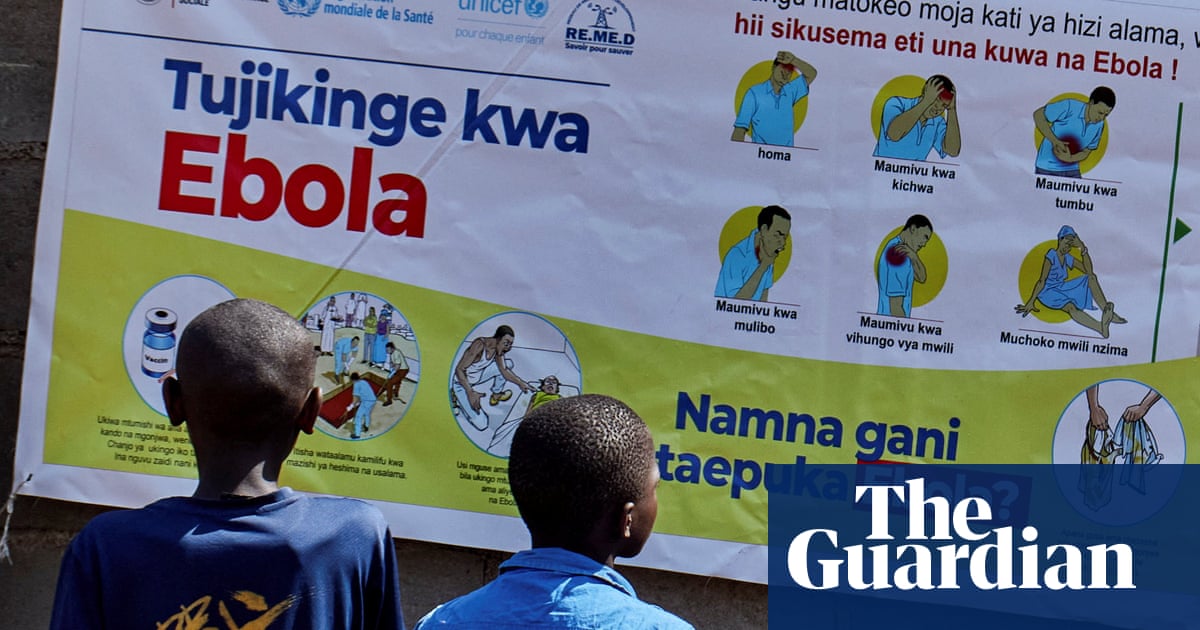
Ebola Outbreak in Central Africa Raises Concerns
A previously unnoticed outbreak of Ebola is spreading in parts of central Africa, while the US seems to be doing little to intervene, following significant reductions in both global and local public health initiatives.
The Bundibugyo variant of Ebola, which lacks a cure or vaccine, has led to two recent outbreaks. Health authorities and scientists are now scrambling to understand its spread and implement measures to counter it, yet the US is notably absent from these efforts.
Over the past year, the US Agency for International Development (USAID) has undergone significant downsizing, with thousands of health agency employees laid off, communication halted, and critical research projects canceled.
Currently, there are 482 suspected Ebola cases and around 116 deaths reported in the Democratic Republic of the Congo (DRC) since April, with additional cases and a death in Uganda, along with potential transmission to South Sudan. Kristian Andersen, a professor of immunology and microbiology, remarked that the outbreak “might have been going on for a few months.”
This outbreak was swiftly declared a public health emergency of international concern by Tedros Adhanom Ghebreyesus, the head of the World Health Organization (WHO). Officials predict that it could persist for several months.
“The DRC has one of the most vulnerable healthcare systems globally, previously receiving substantial funding from USAID,” said Matthew Kavanagh, director of the Center for Global Health Policy and Politics at Georgetown University. He noted that the unexpected withdrawal of US funding has disrupted fundamental health activities in the country.
US foreign assistance to the DRC fell dramatically from $1.4 billion in 2024 to just $431 million in 2025, with only $21 million allocated thus far this year. Similarly, funding for Uganda decreased from $674 million to $377 million last year, with negative allocations reported in 2026.
Andersen pointed out that global health investments are relatively inexpensive, arguing it’s much easier to prevent outbreaks than to respond to them. With the US discontinuing preventive measures, the likelihood of reactive scenarios increases.
The US also announced its withdrawal from the WHO and the termination of $130 million in funding, leading to a loss of over 2,300 jobs within the organization. Kavanagh criticized these cuts as self-sabotaging, emphasizing the foreseeable consequences of diminishing public health resources.
“We’re not just stepping back; we’re completely pulling out of the dialogue,” Andersen added. “It’s as if we’re entirely upending the table.”
The Centers for Disease Control and Prevention (CDC) has historically led in healthcare responses but saw a suspension of Ebola response teams and essential supplies under the previous administration.
A specialized Ebola lab in Maryland was ideally positioned to aid in this situation. Normally, it would be engaged in testing potentially effective treatments and vaccines against the current strain, but its operations were abruptly stopped last year, and its website suggests it remains inactive.
During a recent press conference, Satish Pillai, an incident manager for the CDC’s Ebola response, stated he “can’t speak” about the NIH lab’s status. Instead, he noted that the US can still conduct Ebola testing via its laboratory network, which didn’t address the question directly.
Currently, numerous essential roles at US health agencies remain unfilled. The CDC lacks a director, and there’s no US surgeon general or commissioner for the FDA. There are reports of only 25 to 30 staff members in the DRC country office, with further personnel being sent from the CDC.
After the abrupt dissolution of USAID, the DRC office faced sudden and large cuts. Former employees filed lawsuits after losing their jobs with no options for evacuation or other support.
“When USAID withdrew its support, many health workers who were monitoring potential spillover in the DRC and Uganda suddenly found themselves without resources,” Kavanagh noted. He emphasized that front-line health workers typically identify outbreaks, as patients do not usually seek care suspecting they have Ebola, but rather present with general symptoms.
This vital work is now being replaced by country-specific agreements, which seem to rely on shared resources. Andersen expressed disapproval, indicating that the US is “holding hostage” nations that have built their health systems based on US guidance and abruptly cutting off support.
Kavanagh remarked that in the past, the US played a crucial role in preventing potential global outbreaks. He added that the failure to detect this outbreak earlier raises questions about the US’s commitment to its role in global health.
Rather than addressing the outbreak constructively, the US has instituted travel bans for noncitizens who have visited the region, which Kavanagh described as ineffective “public health theater.” The Africa CDC urged countries to avoid “fear-driven” travel restrictions, highlighting that the most effective way to protect people globally is by supporting outbreak control at its source.
As it stands, this epidemic is spiraling out of control, potentially leading to more deaths and a significant crisis in the region. Kavanagh acknowledged that local health leaders in the DRC are knowledgeable and experienced, but they face severe limitations due to hefty cuts in global support.
Andersen added that African scientists have conducted impressive sequencing work already, which may unravel the outbreak’s origins. However, he cautioned that this doesn’t justify the US isolating itself from global efforts.
Such outbreaks pose serious implications for economic, geopolitical, and global stability. Kavanagh stressed that allowing preventable deaths from curable diseases is immoral. He concluded, “Ebola can indeed be stopped, but mobilizing resources and public health efforts is essential. The question isn’t whether it can be stopped, but if it will be and when.”