Situation at a glance
On January 26, 2026, Ethiopia’s Ministry of Health announced the end of the Marburg virus disease (MVD) outbreak. This decision followed two full incubation periods—42 days—after the last confirmed case, who passed away and received a proper burial according to WHO guidelines on December 14, 2025. By January 25, 2026, a total of 19 cases had been confirmed, which included 14 confirmed cases (nine of those resulting in death) and five probable cases, all fatal. Monitoring for 857 contacts was successfully completed during this period.
WHO, alongside its country office and partners, played a crucial role by providing technical and financial assistance to help the government manage the outbreak effectively.
Description of the situation
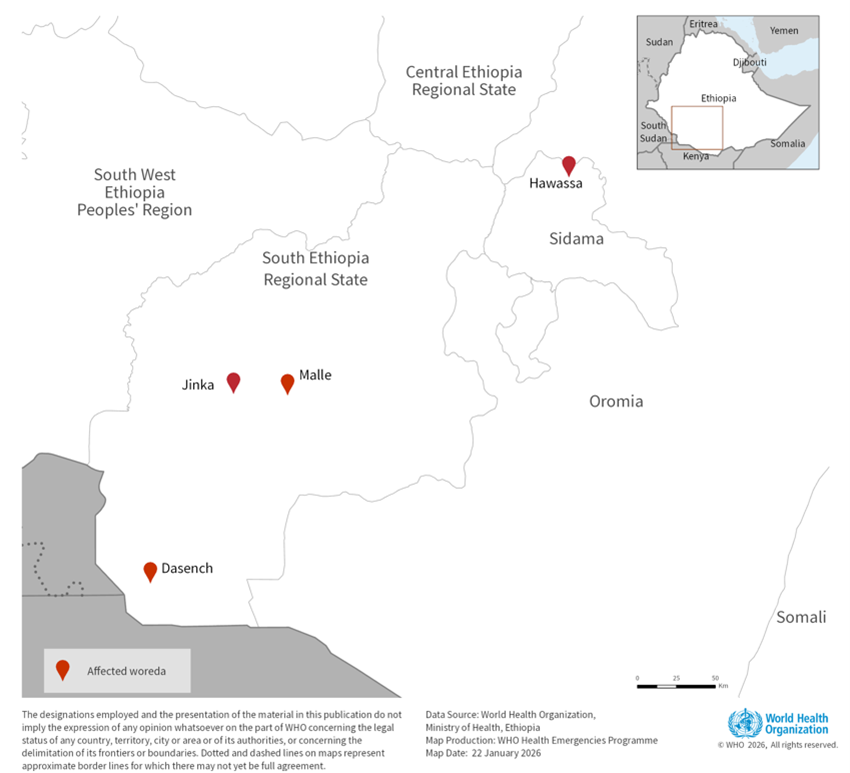
On November 14, 2025, following the confirmation of suspected viral hemorrhagic fever (VHF) cases in Jinka, Ethiopia, the country’s Ministry of Health declared a Marburg Virus Disease outbreak. Testing by the National Reference Laboratory identified the Marburg virus in samples from patients. This marked Ethiopia’s first reported MVD outbreak.
The outbreak began with a case from Jinka town, where the individual showed symptoms starting October 23. The person sought medical attention the next day, exhibiting symptoms like fever, vomiting, and abdominal pain. As of January 25, 2026, the total included 14 confirmed cases with nine deaths (a Case Fatality Rate of 64.3%) and five probable fatalities in the South Ethiopia Region and Sidama Region.
By January 25, 2026, 857 contacts had completed the required 21 days of monitoring, comprising 760 from South Ethiopia and 97 from Sidama. Additionally, 3,800 samples had been tested by January 5, 2026.
On January 26, 2026, after the completion of two incubation periods without any new confirmed cases, the Ethiopian Ministry of Health declared the MVD outbreak officially over, adhering to WHO protocols.
Epidemiology
Marburg virus disease is a severe condition caused by either the Marburg virus or the Ravn virus. Historically, MVD has a high case fatality rate, varying between 24% to 88% during past outbreaks, though early treatment can reduce this risk. It mainly transmits to humans through fruit bats and subsequently spreads via direct contact with bodily fluids or contaminated surfaces. Healthcare workers and caregivers are at heightened risk if appropriate infection control precautions aren’t adhered to.
Symptoms usually appear suddenly after an incubation period of 2 to 21 days, manifesting as high fever, severe headaches, and progressively worsening gastrointestinal issues like diarrhea. In the most severe cases, bleeding occurs from multiple sites, leading to death within a week of symptom onset.
Currently, there are no approved vaccines or treatments for MVD, although early supportive care can enhance survival rates. Some potential vaccines and treatments are still under investigation.
Globally, 19 outbreaks of MVD have been documented, with the latest reported in Tanzania from January to March 2025. Other countries in Africa that have witnessed MVD outbreaks include Angola, the Democratic Republic of the Congo, Equatorial Guinea, and several others.
Public health response
Ethiopian health authorities at both local and national levels executed several public health measures:
- A National Taskforce was set up at the Ministry of Health for strategic decision-making and resource mobilization.
- A detailed three-month response plan was developed and enacted by the MoH and EPHI.
- The MoH ensured that public information on the outbreak was regularly shared with citizens and stakeholders.
- Operational Centres for Public Health Emergencies were activated to coordinate the response at both national and regional levels.
- Collaborative surveillance and response activities were conducted in coordination with regional health offices, especially at critical entry and control points.
- Efforts for community surveillance, contact tracing, house visits, and healthcare services were intensified.
- Two hospitals were designated as treatment centers staffed by health workers trained to manage cases.
- Laboratory facilities were enhanced nationally, with a mobile lab deployed in Jinka for prompt confirmations.
- Field assessments were carried out by a rapid response team.
- Risk Communication and Community Engagement teams worked on delivering prevention messages, addressing misinformation, and enhancing public awareness through local influencers.
WHO, with various partners, also provided vital support, including:
- Technical and operational guidance across all response sections.
- Emergency supplies such as testing kits and treatment center modules.
- Deployment of experts for operational assistance.
- Support for capacity building in surveillance and case management practices.
- Assistance in integrating the MVD response into essential health services.
- Community-based initiatives for active case finding and mortality tracking were also supported.
WHO risk assessment
This was Ethiopia’s inaugural confirmed MVD outbreak. Continuous monitoring and investigative activities—including contact tracing and case management—indicated no additional cases during the 42-day observation period as stipulated by WHO. However, there remains a possibility for MVD to re-emerge due to potential spillovers from animal reservoirs.
Ongoing risk communication and community outreach will be crucial for providing timely information, addressing community concerns, and reducing stigma associated with those affected.
WHO advice
WHO emphasizes the importance of maintaining early detection and care capacities, along with the ability to respond swiftly if the outbreak resurfaces. This preparedness is vital for immediate identification and prevention of further spread, which can save lives.
Raising awareness about MVD risk factors and preventive measures is essential in reducing transmission. WHO recommends the following protective strategies for healthcare settings and communities:
- Avoid prolonged exposure to mines or caves where fruit bats live and use protective gear if entering these areas.
- Maintain capabilities for the early detection of MVD cases in at-risk settings.
- Prevent human-to-human contact with infected persons, ensuring those suspected or confirmed of MVD are treated in designated facilities.
- Communities should keep well-informed about the disease and containment strategies.
- Measures should include respectful burial protocols, health monitoring for contacts, and prompt referral of symptomatic individuals to healthcare facilities.
- Implementation of critical infection prevention practices in healthcare settings is essential, including the safe handling of waste and appropriate hygiene protocols.
- Ensure that patient care occurs in environments that support infection control practices and access to safe water, sanitation, and hygiene.
- Encourage comprehensive support for MVD survivors, addressing potential health repercussions and providing access to testing for body fluids.
Currently, WHO does not recommend any restrictions on travel or trade with Ethiopia.
Further information
Citable reference: World Health Organization (January 26, 2026). Disease Outbreak News; Marburg virus disease in Ethiopia. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON592