Did John Nash Really Have Schizophrenia?
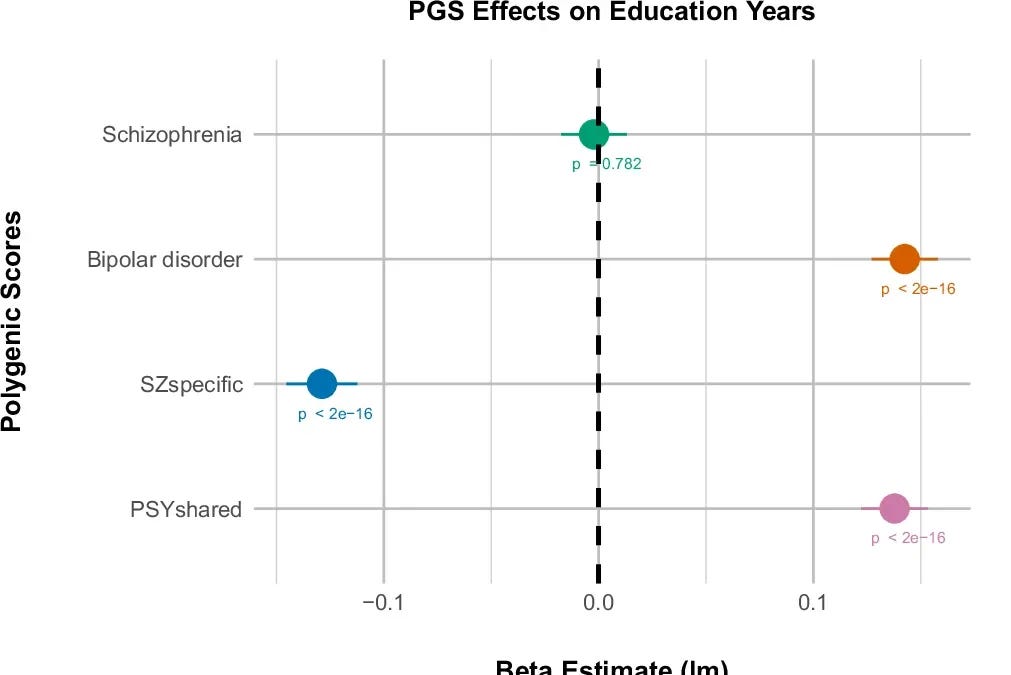
Michael Halassa published an intriguing piece on the genetics behind psychosis. Previous studies indicated that while genes associated with schizophrenia tend to lower IQ, they also correlate with greater educational achievement. This finding was unexpected, given the typical relationship between IQ and education. New research identifies two layers of genetic risk linked to schizophrenia. The first, which overlaps with bipolar disorder, is associated with increased educational attainment. The second, unrelated to bipolar disorder, appears to reduce IQ. Together, these factors result in a genetic profile that reflects stable to increased educational attainment alongside stable to decreased IQ.
Back in 2021, I touched on the topic of tradeoff versus failure models in psychiatric conditions, suggesting that many issues likely embody a blend of both. The latest findings seem to corroborate this view: the initial genetic risk for schizophrenia represents a tradeoff—while it heightens the risk of developing the disorder, it also fosters better educational outcomes. This could be linked to aspects like creativity or drive. In contrast, the second component seems purely detrimental, offering no redeeming benefits. It may stem from harmful mutations in genes involved in neurogenesis and synaptic pruning.
Interestingly, I hadn’t considered schizophrenia in my earlier discussion about tradeoffs and failures, so I was somewhat taken aback by how well this theory aligns here. But looking back, it seems pretty logical. Many complex issues should logically involve elements of tradeoffs and failures.
Let’s think about something relatable like poverty. Some individuals may experience poverty due to “failures”—traits that bring no balancing positives. They could be less intelligent, suffer from chronic illnesses, or live in underprivileged areas with subpar education. In these scenarios, something has malfunctioned—be it their health or educational systems.
On the other hand, some people might be poor due to tradeoffs. Consider the aspiring artist who forgoes a stable job to chase their creative aspirations, or the bohemian who opts for a laid-back lifestyle over the eight-to-five grind. These individuals generally have an average chance for success, but they purposefully allocate their resources in ways that yield less financial gain in exchange for other fulfilling experiences.
We could apply this idea to a range of negative experiences. For instance, someone might be single due to being unattractive and socially awkward, or they might have consciously traded the benefits of a relationship for freedom and casual encounters. A disappointing pizza might be the result of a chef’s incompetence, or perhaps it traded off taste for lower cost, convenience, or dietary concerns like veganism or gluten-free options. It’s all relatively straightforward when we look at common situations, like dating or food. The essential realization here is that these are multi-dimensional landscapes, where a variety of factors can influence outcomes, and many of them likely fall into the categories of “by choice” and “not by choice.”
Physical health issues reflect a similar dynamic. Take cancer—it’s a breakdown in the normal processes that regulate cell growth, and various risk factors underscore this: exposure to radiation, pollution, or genetic mutations. Yet, there’s also a tradeoff involved: often, higher cancer risk correlates with lower chances of developing certain degenerative diseases, like Alzheimer’s. This could be due to the delicate balance between promoting cell division for healing and staving off cancer risks.
If we extend this concept, even having a limb amputated can involve both types of risk. Maybe someone loses their leg due to sheer bad luck—say, tripping over something— or they might lose it because they prioritized bravery and honor in battle over their own safety.
This doesn’t imply that this pattern applies universally. If taken too literally, one could mistakenly believe that any condition must come with certain advantages, while in reality, it’s the risk factors associated with those conditions that may carry some benefits. For instance, although cancer is generally harmful, it’s not ideal to keep one’s body in a state that minimizes cancer risk at all times. Additionally, conditions that are too simplistic to fit into this multifactorial framework don’t necessarily exhibit both tradeoff and failure attributes. For example, muscular dystrophy appears to be simply negative, probably due to the size of the gene responsible for muscle protein—thus increasing the odds of random mutations.
Previously, I framed the combination of tradeoff and failure in psychiatric conditions as a complex issue. Now, I feel that I’ve clarified it to the point of feeling almost foolish for having made such a big deal of it before.