Public Health Updates: What’s Happening This May
Bugs may have ears, but this May has been full of loud warnings for public health. We’ve seen everything from explosions at chemical plants to outbreaks of Ebola and hantavirus, not to mention the normal challenges like colds, ticks, and heat stress.
With the World Cup just about two weeks away—who’s counting, right?—we’re busy preparing our Health Security Operations Center for what promises to be a vibrant, albeit hectic, celebration of global culture. It’ll take a concerted effort to keep everyone healthy, involving communities, individuals, and healthcare systems.
And that’s where you step in.
If you plan to attend any games or are within 30 miles of a stadium, we’d really like to hear from you. Consider signing up for a weekly survey here. Huge thanks to the over 1,280 folks who’ve already joined. We’ll be reaching out soon.
On the global stage, the number of hantavirus cases linked to cruise ships has now climbed to 13, with 11 confirmed and three fatalities. The new cases are among individuals who were already in quarantine:
-
A crew member located in the Netherlands.
-
A passenger from Spain, also quarantined at home, tested positive while under observation and has since been admitted to a biocontainment unit.
As for the U.S., no one has tested positive yet. However, with an incubation period of up to 45 days, we may see more cases emerge soon. Thankfully, by May 29, we reach a median incubation window of 18 days.
What this means for you: Your risk from this outbreak remains very low at the moment.
A special thanks to Dr. Craig Spencer, a physician with experience treating Ebola, for updating everyone on the situation.
Currently, the total combined count of confirmed and suspected Ebola cases in DRC exceeds 1,000. Signs suggest a prolonged and severe outbreak:
-
This is likely an undercount. The test positivity rate is around 50%, and only 20% of contacts are being traced. Many new cases are appearing without known connections, implying community spread is likely occurring.
-
It’s still very early in the detection phase. In comparison to past outbreaks, this one is escalating quickly. Remember the 2016 West Africa outbreak that began with 49 cases and grew to 208 in a month? That took four months to match the current numbers in DRC.
-
The cases are widespread. We now have multiple epicenters across 16 health zones, complicating containment efforts.
In neighboring Uganda, there are currently seven cases. While small, the situation has grown concerning with two healthcare workers testing positive without a clear exposure history, indicating potential undetected spread.
On the ground, there’s been backlash against health centers, reflecting a profound and deep-rooted distrust within communities. This often stems from external teams working without comprehending local needs. It’s vital for community trust to be built well ahead of any crisis.
U.S. priorities seem clear, but may have unintended consequences. The administration’s top focus appears to be keeping Ebola out rather than helping contain the outbreak in DRC, resulting in strict travel restrictions that may hamper efforts to trace those potentially exposed.
For example, high-risk American travelers might face mandatory quarantines before returning home, with infected individuals sent to a hospital being set up from scratch in Kenya. This is much more stringent compared to previous responses.
On the surface, these precautions seem sensible, but they could cause issues:
-
Restrictions like these may encourage people to hide where they’ve been, making tracking harder.
-
They also foster a false sense of security, promoting the idea that these issues are someone else’s problem.
-
Ultimately, lives could be lost. The current Ebola strain has no treatment, relying heavily on health system infrastructure, which we have but are not utilizing for infected Americans.
It’s frankly frustrating. The only effective way to minimize risk for everyone is to stop the outbreak in DRC and surrounding areas.
What this means for you: If you have any travel plans to this region, you should reconsider. It’s a high-risk situation, as indicated by the CDC’s Level 4 Travel Advisory. Plus, uncertainty about returning remains high.
For the general public in the U.S., your current risk remains extremely low.
In some good news for those in the Northeast and Midwest, tick populations are continuing to decline, which is a pleasant surprise given it’s peak season.
As for heat risks, they’re not yet widespread, but this week they will be moderate in the Midwest and Southeast.
What this means for you: Be sure to use the CDC’s HeatRisk tool. If it’s a red day, maybe it’s not the best idea for your asthmatic child to play soccer, and orange days may be a good time to check on elderly neighbors.
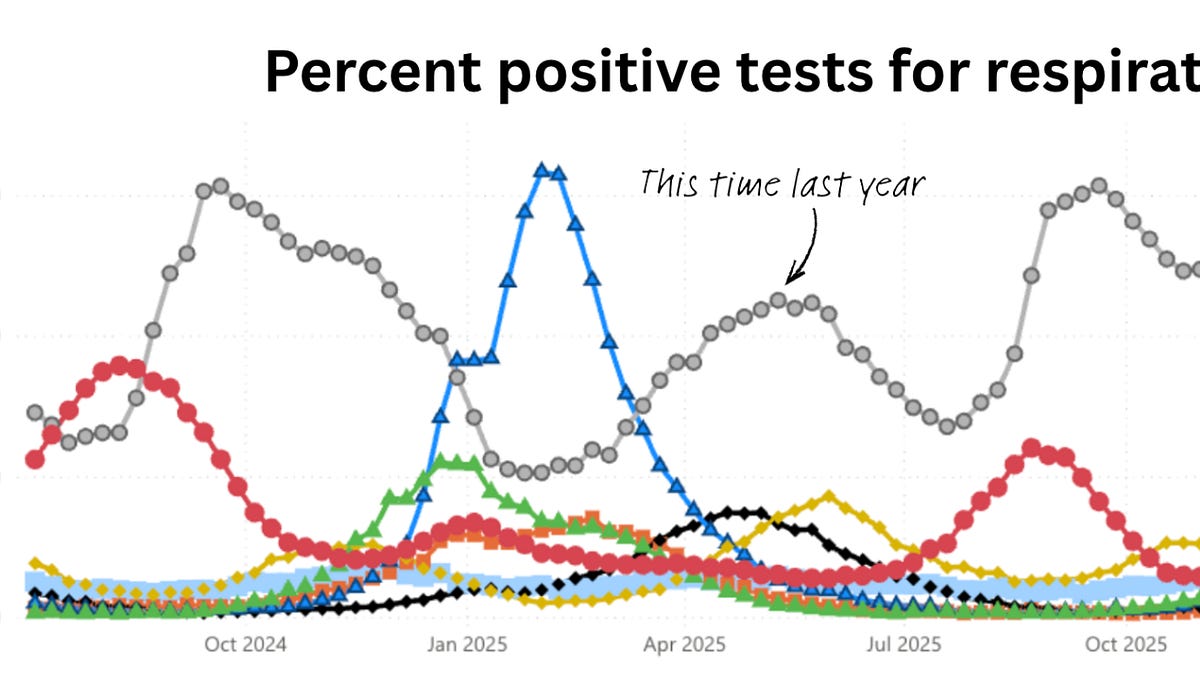
Currently, the common cold seems to be the only respiratory virus on the rise. Although infections are higher than last year, it’s expected to peak soon, with a return anticipated this fall.
Over the weekend, YLE California reported on a serious incident at a chemical plant in Orange County. Fortunately, the worst-case scenario—a chemical explosion—was thankfully avoided, though it might have been sheer luck. The health implications in such a dense population could have been dire.
Then, another explosion occurred in Washington State, which tragically resulted in fatalities. Health officials are saying the risk level for local residents remains low, but the community is entitled to more transparency.
Americans often rank clean air and water as top public health concerns, yet responses to chemical disasters typically fall short on transparency, offering reassurances instead. For instance, residents affected by the 2023 train derailment in East Palestine, Ohio, are still lacking clear answers about the potential long-term health impacts.
What this means for you: Many are rightfully concerned about whether facilities handling hazardous materials are nearby. You can use this interactive map to enter your ZIP code and check the EPA’s list of monitored facilities, including any violations.
-
Vaccines for the Bundibugyo strain of Ebola are in the works. Two different platforms are being developed, one of which may be available within two months. One vaccine is from Oxford, while the other uses similar technology as the FDA-approved Zaire strain of Ebola. There’s potential for cross-protection, though it remains unclear at this stage. Additionally, there are two monoclonal antibody treatments likely to be deployed, although limited doses and significant logistical challenges are hurdles.
-
PCOS is now officially known as polyendocrine metabolic ovarian syndrome (PMOS). This change, decided after a decade of deliberation among about 22,000 professionals and patients, can help reduce misconceptions surrounding the condition, especially for those without visible cysts. The WHO estimates that 70% of those with PCOS are undiagnosed, so a more accurate label can help empower better recognition and treatment.
Public health challenges seem to be everywhere, highlighting the need for dedicated professionals working tirelessly behind the scenes, along with each of us stepping up for our communities.
Best regards, YLE
A big thank you to Ed Nirenberg for his vigilance on Ebola vaccines, to Hannah Totte for all the figures, to Dr. Craig Spencer for his Ebola insights, and to Dr. Matt Willis for covering the chemical situation in California.