








Measles Outbreak Raises Concerns About U.S. Immunization Status
In the early 1960s, American children queued for their first measles vaccines, and it took nearly four decades to build robust immunization programs. By 2000, experts declared that measles had been eliminated in the United States.
For 25 years, outbreaks were few and far between, mainly occurring when infected travelers brought the virus from other countries. Typically, these outbreaks lasted less than a year.
However, times have changed.
In January of last year, measles resurfaced dramatically in West Texas, with cases spreading to nearly every state. Tragically, two unvaccinated girls from Texas and an adult in New Mexico died as the outbreak showed signs of dwindling by July.
As the outbreak faded, infections appeared in Utah, yet health officials struggled to trace the origins of these new cases. Spread in Utah accelerated during the fall and winter, continuing into May of this year.
This situation has opened up a complicated and politically charged question: Could the U.S. lose its measles-free status?
While countries aren’t penalized for losing this designation, it indicates significant issues within a country’s immunization programs and possibly a decline in public trust regarding vaccines.
To maintain its measles-free standing, the U.S. must convincingly demonstrate that the virus did not spread continuously within its borders for over a year. For instance, if the Texas strain crossed into Utah and continued to infect people, it would be problematic. In contrast, if cases in Utah stemmed from a traveler who contracted measles overseas, it could restart the timeline.
The Centers for Disease Control and Prevention (CDC) is examining the full genetic makeup of the measles viruses affecting patients to find clues. A review in November indicated that the Utah cases were likely not genetically linked to those in Texas. However, a spokesperson mentioned that a more extensive investigation is ongoing.
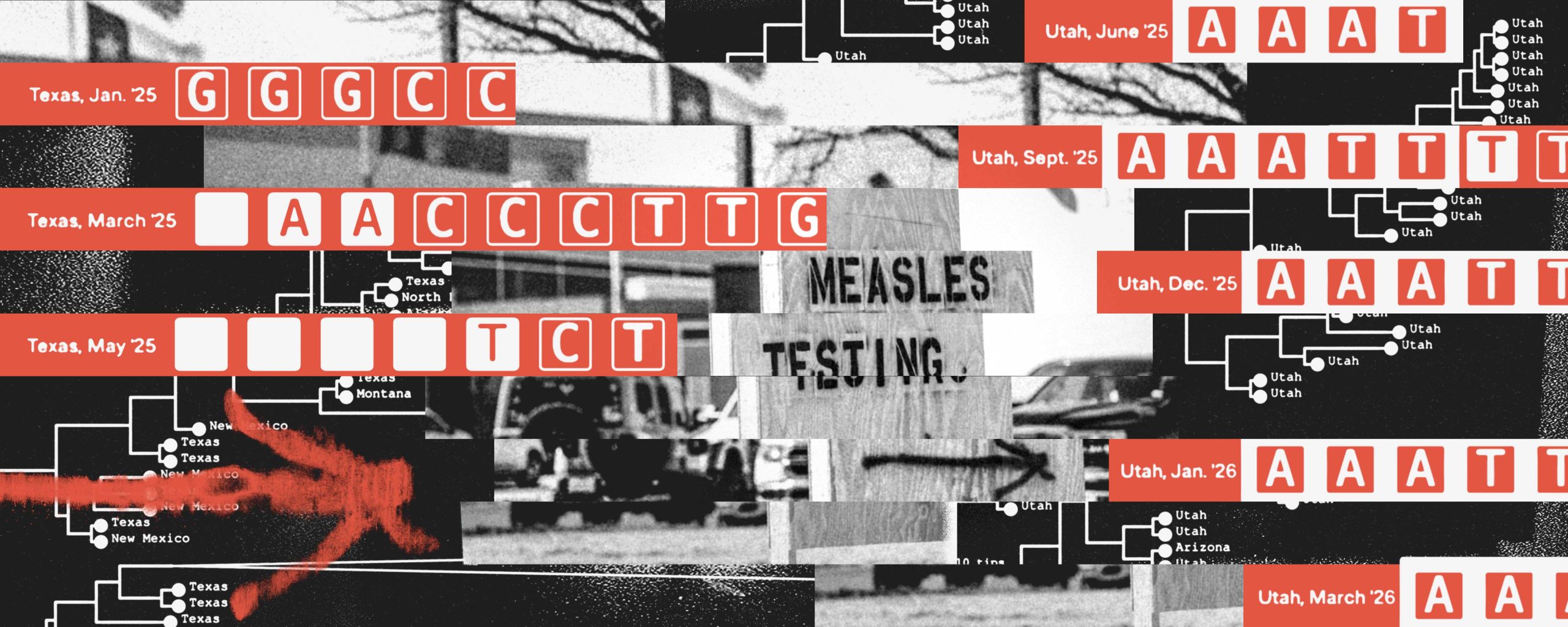
In a separate analysis, ProPublica examined over 1,800 whole genome sequences, revealing that the measles virus still circulating in Utah this May closely resembles the one that affected Texans over a year ago.
While these findings are concerning, they don’t offer definitive proof of endemic spread. Determining whether the virus spread internally or was reintroduced by a traveler remains unclear.
Given the genetic similarities identified, experts believe the U.S. might struggle to argue that measles isn’t endemic, unless the CDC uncovers new evidence, as suggested by Dr. Alberto Severini, a retired molecular virologist.
These unique genetic mutations aren’t confined to Texas and Utah. Similar mutations have been found in cases in Iowa, North Dakota, Minnesota, and Alaska. However, genomic sequencing from cases in Mexico or Ontario hasn’t been made public, which complicates the situation further.
This matters because determining whether the virus has been continuously circulating in the U.S. is crucial for a panel from the Pan American Health Organization (PAHO) that will decide on the U.S.’s measles-free designation.
Canada lost its designation last year. PAHO invited the U.S. to present its case in April, but officials requested more time to investigate. The review has been pushed to November.
Daniel Salas, a PAHO official, noted that a thorough genomic analysis takes time as the CDC looks for patterns that might show when and where mutations occurred.
One of the significant mysteries is how measles reached Utah. Authorities found that the state’s first confirmed patient last June could not have been exposed to the virus abroad or in another state. Despite their efforts, health officials still couldn’t pinpoint where the infection came from.
Cues suggested that measles may have been quietly spreading in the area. Investigators noted reports of community members with rashes last June, though many declined testing and families were hesitant to cooperate.
No interviews indicated that any patients were exposed internationally, according to Dr. Leisha Nolen, the Utah State Epidemiologist. Yet, she couldn’t dismiss that possibility.
ProPublica inquired whether the CDC had linked any Utah measles cases to an international outbreak, but the agency refrained from providing details or commenting on the genetic similarities found. They emphasized that sequencing alone cannot confirm continuous transmission.
As the midterm elections loom, the measles resurgence poses a political challenge for President Trump. Under his leadership, there have been over 4,300 cases—figures not seen in thirty years.
Eliminating endemic measles is an arduous public health challenge given its highly contagious nature. The virus can be infectious before the telltale rash, lingering in a room for hours.
Previous U.S. outbreaks prompted robust immunization initiatives—states mandated vaccinations for school and daycare entry, with federal programs providing free vaccines to low-income families. When measles resurfaced, states like California and New York tightened school exemptions, reinforcing a commitment to vaccination.
Health leaders used to urge parents to vaccinate their children, assuring them of the vaccines’ safety. However, Trump and HHS Secretary Robert F. Kennedy Jr. have both raised doubts about the MMR vaccine, which protects against measles, mumps, and rubella.
Despite extensive global research indicating the vaccine does not cause autism, Trump raised concerns about the combination vaccine at a press conference, advising parents to seek separate shots—a claim complicated by the absence of such options in the U.S. Kennedy stated that while the vaccine protects against measles, he has often framed it as riskier than the disease itself.
Measles results in fatalities for 1 to 3 in every 1,000 infected individuals and can lead to serious complications like deafness and encephalitis. The Infectious Diseases Society of America notes that healthy individuals have not shown vaccine-related deaths, although rare adverse events have occurred in immune-compromised children.
HHS spokesperson Andrew Nixon stated that Kennedy believes Americans deserve clear information on medical procedures. He argued that distrust in health institutions grew during the pandemic due to mandates and suggested rebuilding that trust through transparency rather than coercion.
Kennedy has attempted to separate himself from the measles situation, insisting that the U.S. has managed the outbreak better than other nations, pointing to higher case numbers in Canada and Mexico.
Furthermore, he noted that the Texas outbreak predates his appointment as health secretary.
Kennedy has been a prominent figure in the antivaccine movement for over a decade, with Dr. Adam Ratner, a pediatric infectious disease physician, criticizing him for undermining vaccine confidence in the U.S.
During a 2018 outbreak in New York City, Ratner treated unvaccinated children who required hospitalization, demonstrating that measles can have severe consequences.
While many parents still support vaccinations, Ratner expressed concern about the diminishing resolve to enforce stricter vaccine requirements in schools, with some states embracing medical freedom instead.
“A highly vaccinated population is essential to control the spread,” Ratner stated, warning that without it, ongoing outbreaks—and even tragedies like those in West Texas—are likely to continue.
The U.S. might find means to prove its measles-free status, but experts caution that it may only be a temporary fix if underlying issues remain unaddressed.
“Transmission has occurred in the U.S. for over a year,” Severini remarked. “If vaccination rates don’t improve, measles will become endemic.”







