








Potential End to Historic Government Shutdown
We might be nearing the end of the longest government shutdown in U.S. history, though nothing is set in stone.
As Congress debates the future of Affordable Care Act (ACA) subsidies, people across all insurance types are preparing for increased premiums, limited network options, and tougher decisions regarding their health care.
The debate in Washington seems somewhat limited to me. The bigger issue isn’t solely whether these subsidies will continue or be cut, but rather how off-kilter our entire health care system has become. It’s crucial to question if there’s a genuine effort to tackle the underlying costs involved.
Teaming up with experts has been essential. One such expert, Hayden Luke-Lee, has pinpointed five reasons that contribute to our system’s current problems.
Let’s delve deeper.
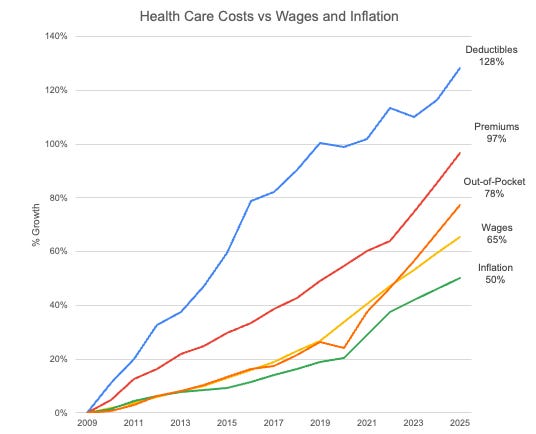
In the last twenty years, costs for employer-sponsored health insurance have surged. For most Americans with private insurance, insurance premiums, deductibles, and out-of-pocket expenses are climbing at a much quicker pace than wages.
This growing disparity means that, even if salaries inch up, workers are effectively earning less. Every dollar spent on insurance is a dollar not available for housing, groceries, or childcare.
The personal toll is evident. One in three Americans faces medical debt, with more than half anxious about accumulating debt every time they access the health care system. Such concerns lead people to delay appointments, skip essential medications, or even completely avoid necessary treatments.
Medical debt has become the most prevalent type of debt in collections, surpassing credit cards and other loans. It’s alarming to note that about 60% of individuals with medical debt actually have insurance.
Despite the U.S. pouring more money into health care than any other wealthy nation, the outcomes are poor. Access is limited, and the morale among workers is decreasing.
The paradox here? Even with unprecedented spending, Americans generally have shorter life expectancies and are more likely to fall ill compared to people in Europe, Canada, and Japan. Rates of infant and maternal mortality, along with chronic diseases, rank among the highest in wealthy countries. A large part of this is due to a heavy investment in specialized services rather than preventive care like primary health services and community support systems.
There’s a common claim that at least there are no long waits for care, unlike in some other countries. However, that narrative is increasingly changing. With all that spending, we’re essentially doubling the costs compared to other nations—and still facing access issues. Nearly 100 million Americans fall into all kinds of care access deserts, including 60 million without adequate primary care or pharmacies. Mental health services are notably scarce, and Medicare doesn’t cover long-term care.
Healthcare workers often burn out or leave the field altogether. Home health aides are notoriously underpaid for their crucial roles. It’s disheartening to see some nurses find themselves competing as gig workers. Many physicians describe feeling demoralized in a system focused more on billing than on treating patients.
There’s a prevalent belief among policymakers that the high costs of care stem from overconsumption. A related theory asserts that doctors provide excessively costly treatments, driven by payment for each service rendered. While some low-value care exists, the reality is more complex. With corporations increasingly owning health systems, they’re continuously finding ways to charge more for a wider array of services.
Yet, many Americans don’t actually use the healthcare system more frequently. It’s striking that both hospital stays and common surgeries, like knee and hip replacements, are on the decline. The main issue? It’s all about price. For instance, a colonoscopy or MRI can differ wildly in cost from one hospital to another, often without corresponding differences in care quality.
This variation stems from a lack of transparency among the tangled web of insurance companies, hospitals, and other intermediary entities. We’ve created a scenario where no one, not even doctors or patients, knows what services will ultimately cost, leading to surprise bills weeks later.
Moreover, the private sector is cluttered with inefficiency and bureaucracy that surpasses that seen in other countries. Each insurance company has its own pricing and processes, which only adds to wastefulness. Nearly a quarter of health insurance spending goes to things other than direct care, like marketing and billing.
Healthcare professionals find themselves burdened with paperwork, while patients spend hours disputing denied claims. This blurs the lines of actual healthcare costs.
Perhaps one of the least acknowledged shifts over the past few decades has been the consolidation of healthcare into corporate hands. Community-based care has largely been replaced by large corporate entities.
Now, we see major corporations like UnitedHealth Group dominating not only insurance but also employment and health services. Similarly, CVS Health, the largest pharmacy chain, has absorbed numerous other healthcare entities. This merger frenzy creates a web of conflicts of interest, leading to higher prices and pushing independent providers out of the market.
Private equity’s involvement in healthcare rose dramatically between 2000 and 2020, growing massively in transaction value. Private equity firms are acquiring everything from nursing homes to physician practices, typically focusing on cutting costs and raising prices before selling for a profit. The evidence suggests that the quality of care diminishes, and sometimes even mortality rates increase after such acquisitions.
This situation didn’t arise by accident. The trends we’re witnessing today started in the 1980s, fueled by a bipartisan agreement to address escalating costs through more free-market approaches in healthcare, resulting in three significant policy changes.
-
Insurance companies now compete for patients, which was thought to lower costs and improve quality. In reality, the government spends billions to support leading insurance companies managing Medicaid and Medicare and ACA exchanges. The same goes for prescription drugs—Medicare does not directly negotiate prices anymore, leaving that to pharmacy benefit managers, which adds extra pressure on Americans.
-
There’s heavy reliance on economic incentives, suggesting doctors and patients can only make informed decisions when there’s competition. While this narrative is often accepted by both major political parties, it overlooks that patients can’t really “shop” for urgent surgeries or treatments.
-
The shift from nonprofit to for-profit healthcare has diluted commitments to community and ethics in service delivery.
The current discussions seem to recycle old strategies, hinting at increased private control and out-of-pocket costs while also reducing regulations on pricing and profits. This approach has not worked over the past forty years and likely won’t work going forward since it fails to address the core crisis: inflated costs driven by exorbitant prices, especially for new therapies and poor management of resources.
The dysfunction of the U.S. healthcare system is glaring. An alternative approach is feasible—if we commit to reforming it in favor of patients, clinicians, and taxpayers. It’s essential to rethink pricing structures, eliminate middlemen, and regain control over care delivery to benefit the community.
Health is a universal concern. We must build systems that function for us, not ones that force us to accommodate our health needs.



