For the third consecutive year, officials eligible for the state’s health benefits program will see premium increases in the double digits. Since 2022, insurance premiums have surged for 59% of local and county workers and 40% of national workers.
A recent report from the state Treasury Department, released Tuesday, forecasts another three years of steep premium hikes. Rising costs and uncertainty could push the program towards a “death spiral.”
This health benefits program caters to 450,000 state, county, and local government workers, plus retirees. The local government segment, which serves 156,000 employees across 689 municipalities, is particularly struggling with shortages.
According to the Treasury report, local government insurance programs are “facing concerns about reduced registration, costs, premiums, and long-term sustainability.”
“Without significant interventions, current trends in inflation regarding enrollment, utilization, and healthcare costs will continue to push premiums to unsustainable levels,” the report warns.
While the local government segment has generated $2 billion in annual premiums, the costs are so overwhelming that the state has lent $258 million since November, with only $138 million repaid.
Weight loss drugs, inflation, greed
The cause of the rising costs remains subjective, varying based on whom you ask.
State treasurer Liz Mooio mentioned during a budget hearing that popular weight loss medications like Wegovy and Ozempic, effective for many, may have unintentional consequences of raising public sector premiums.
Moreover, the usage of health insurance, particularly for outpatient services, remains steady, Mooio observed. Most medical procedures come with escalating costs.
The demand for GLP-1 drugs, however, is remarkable. According to a report from Optum RX, the state pharmacy benefits manager, drug use has doubled compared to the previous year.
Optum RX’s analysis reveals that, from January to September 2024, these drugs will cost approximately $286.5 million, shared between worker co-payments and government contributions. Workers only pay around $16 monthly, which means governments shoulder two-thirds of the expenses.
Union leaders representing public servants recognize the high popularity and costs of these drugs but argue they aren’t the primary drivers of expenses.
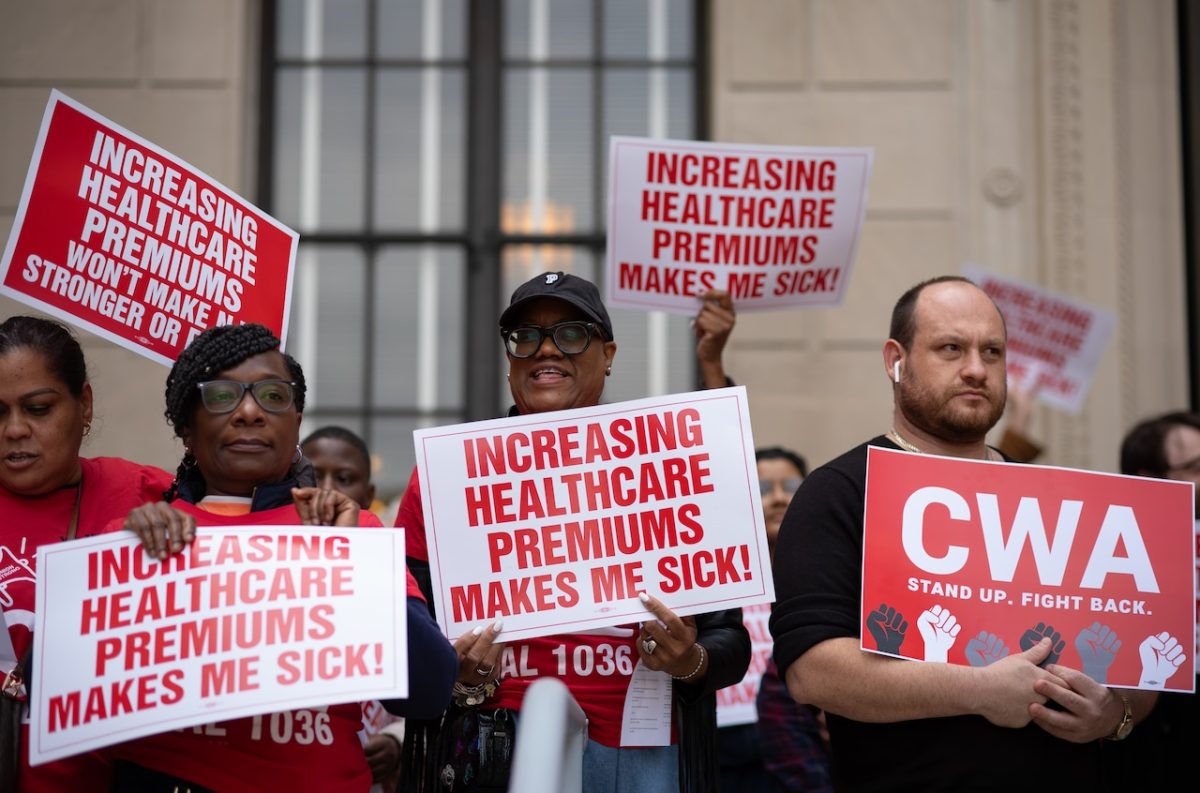
Tammy Carr, vice president of CWA Local 1084, accused hospitals, doctors, and healthcare providers of driving up costs.
“It’s essentially about greed,” she said, addressing a crowd of around 150 union members at a protest in Trenton last month. Some colleagues are paying as much as $1,000 a month in premiums, according to her.
“We have a problem rooted in a broken promise,” Carr declared. “Once upon a time, healthcare was seen as a perk, an essential factor in attracting dedicated public service employees. We were assured that if we committed to our community, affordable healthcare would be available for our families here in New Jersey.”
“It’s not about better care or improved outcomes; it’s really about greed pushing costs to excessive levels,” Carr noted, expressing her frustration.
While she doesn’t deny that the health insurance package offers decent benefits, the financial burden remains significant.
The average annual cost of public worker compensation in New Jersey hit $22,000 in 2023, which is 60% higher than the average across private and public sector plans nationwide.
New Jersey is among just 11 states that include weight loss medications in their employee coverage.
No one has so far suggested dropping this coverage, even though these medications might help reduce risks for heart disease.
But for employees and government workers to escape the impending increase in premiums, something has to change.
Ward Sanders, president of the New Jersey Health Planning Association, brought up issues like the overutilization of robust benefits packages and a lack of financial accountability in service use.
Another significant concern, Sanders pointed out, is how local governments can join or exit the program.
The Treasury report highlights the problem further, citing that many municipalities and agencies have withdrawn from state programs in search of cheaper options.
Approximately 372 local and county employers have left the program, based on the latest figures from the Treasury.
Some towns have sought better deals, as health costs continue to rise and those with existing conditions become more expensive to insure. Each employer is expected to prepare for potential surpluses or claims, but last year, all reserves were depleted, according to the report.
There might be solutions, but time is running out
The union is advocating for a bill that could adjust premiums based on employee pay percentages.
Senate President Nicholas Skutari and Congress President Craig Cofflin opted not to comment on the union’s proposition.
Cerra, a Municipal Federation member, noted that only the Planning and Design Committee alongside the state legislature can make changes, which is problematic.
“We want a seat at the table; however, that doesn’t seem quite right,” Cerra explained. “We participate in meetings and listen in on calls, but we lack the opportunity to influence the process.”
When ideas for reform were previously discussed, the committee faced deadlock due to equal numbers of union and employer representatives.
Cerra emphasized the need for investigation into high prescription drug costs. “Why aren’t economies of scale working for us?”
The Treasury report suggests various measures to alleviate the program’s ongoing challenges, but implementation will require action from the legislature and the committee managing the program.
One proposed long-term approach could phase out the local government segment of the program, transitioning to self-governing groups with state assistance.
Another suggestion is to require local governments that exit to wait 3-5 years before rejoining the state’s plan, helping to minimize the volatility and drastic price increases that often accompany returns. Recently, a bill was put forth to impose this five-year waiting period.
The report also advocates for local governments to maintain a two-month surplus in billing payments to avoid operating at a loss.
“Even the most comprehensive planning changes alone won’t suffice to halt the ongoing systematic unraveling,” the report concluded.